

Background
Multiple Myeloma (MM) is a malignancy of terminally differentiated B lymphocytes (plasma cells, PCs) characterized by secretion of immunoglobulins and/or light chains (LCs). Association of immunoglobulin isotypes with survival in the context of contemporary therapies and accounting for modern prognostic factors has not been determined.
Methods
We utilized the Flatiron Health Electronic Health Record (EHR)-derived de-identified database to source patients (pts) with newly diagnosed MM from 01/2011 to 02/2020 with documented isotype data as part of the initial diagnostic work up. This nationwide database comprises de-identified, longitudinal patient-level demographic, clinical, and outcomes data curated via technology enabled abstraction. We used self-reported race and ethnicity and constructed a composite race/ethnicity variable as used by the National Cancer Institute. Similarly, we defined baseline labs (hemoglobin, serum creatinine, calcium, LDH) as those available within 90 days of diagnosis. We compared baseline characteristics using appropriate bivariate methods. Finally, we used Kaplan-Meier methods and Cox proportional hazard regression models to compare overall survival (OS), from the date of diagnosis, among the different isotypes (IgA, IgD, IgM, Light Chain (LC), others) with IgG MM after adjusting for known prognostic variables such as FISH abnormalities, ISS, renal function, age, sex, race/ethnicity, LDH, ECOG performance status, and treatment.
Results
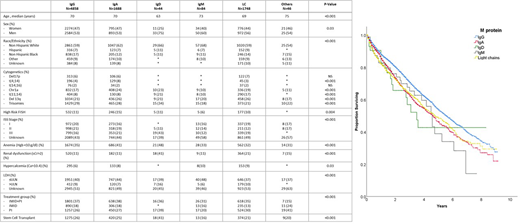
We identified 8468 patients in the database who met the inclusion criteria. Patient with IgA MM (N=1688) were more likely to have ISS-III (IgA 21% vs. IgG 16%, p<0.001), anemia (IgA 41% vs. IgG 35%, p<0.001) and t(4;14) (IgA 8% vs. IgG 4%, p<0.001) than patients with IgG MM (N=4858). LC MM (N=1748) have more renal dysfunction (LC 21% vs. IgG 11%, p<0.001) and t(11;14) (LC 17% vs. IgG 8%, p<0.001).
Patients with IgD MM (N=44) were younger, more likely to be male and non-Hispanic White, have ISS-III, high LDH, anemia and renal dysfunction and t(11;14). Patients with IgM MM (N=84) had higher incidence of hypercalcemia and lower proportion of patients with high LDH (Table). Across all groups 3106 (36.7%) patients received therapy containing a proteasome inhibitor (PI) and an immunomodulatory agent based triplet (IMiD), while 1458 (17.2%) received IMiD-based doublet, 2284 (27.0%) PI-based doublet, and 2109 (24.9%) received hematopoietic cell transplantation. Patients with IgA (mOS 4.7 vs 5.6 years, p<0.001) and LC MM (4.8 vs. IgG 5.6 years, p<0.001) patients have inferior OS (Figure). The adverse prognostic impact of IgA (HR 1.2, 95% CI 1.1-1.3, p<0.001) and LC isotypes (HR 1.2, 95% CI 1.1-1.3, p<0.001) on OS persisted even after adjustment for FISH abnormalities, ISS stage, renal function, age, sex, race/ethnicity, ECOG performance status, LDH, and treatment.
Conclusion
Using a contemporary "real world" dataset, we illustrate the distinct clinical features of MM with different immunoglobulin isotypes. Our findings suggest that IgA and LC MM are associated with poor survival suggestive of their unique biology beyond presence of high-risk FISH abnormalities and other adverse prognostic factors.
Costa:Sanofi: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding; AbbVie: Consultancy; Genentech: Consultancy; BMS: Consultancy, Honoraria; Celgene: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal